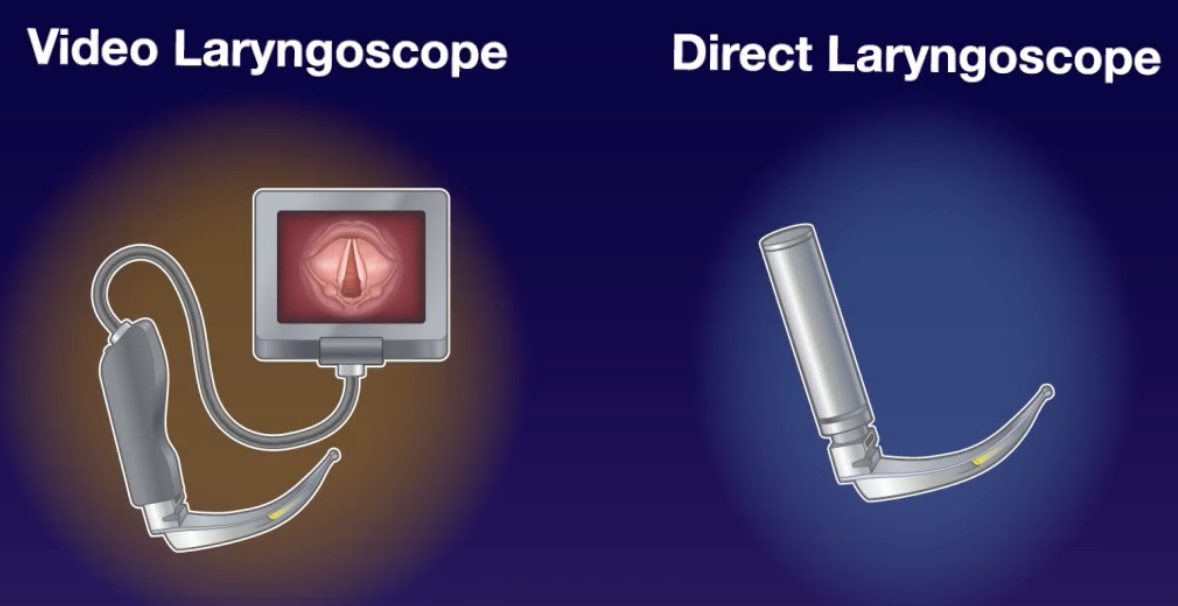
Conclusion: Video laryngoscopy resulted in a greater number of successful intubations on the first attempt than direct laryngoscopy among neonates requiring urgent intubation
My take away: This study adds the neonatal string to the bow of video laryngoscopy, which should be used first-line and as standard of care in all intubations
- Video laryngoscopy has been shown to result in greater first-pass success during intubation and reduce complications for both adults (DEVICE trial 2023)[1] and children (VISI trial 2020)[2]
- Most neonatal intubations occur in the operating room or NICU, and the overall incidence of neonatal intubation has decreased in recent years due to increased use of non-invasive ventilation. A recent retrospective multi centre study reported VL was used during only 23% of intubation attempts in the NICU. Experience in neonatal intubation is often lacking for emergency physicians.
- Attempts at neonatal intubation with DL are successful less than 50% of the time[3]
- This is a single-centre, randomised trial conducted in Dublin looking to determine whether use of VL would result in increased first-pass success for urgent intubation in neonates
- Participating doctors received training in both DL and VL techniques including practise on mannequins from the trial team
- Neonates of any gestational age in whom intubation was attempted either in the operating room or NICU were eligible for inclusion. Only neonates who had upper airway anomalies were excluded
- Most intubation attempts were made by doctors-in-training who were permitted up to 3 intubation attempts, and the supervising neonatologist could attempt intubation at any time at their discretion
- Neonates received induction medications (typically fentanyl, atropine and suxamethonium) in the NICU if time permitted, and generally did not receive in auction medications in the operating room due to lack of IV access. Uncuffed tubes were used. Stylets were used at the discretion of the treating clinician. No supplemental oxygen was used during intubation attempts in either group.
- Both straight and curved blades were available for use in both the VL and DL groups, left to clinician choice
- Primary outcome was successful intubation on the first attempt as confirmed by colourimetric EtCO2 (with an intubation attempt defined as the introduction of the laryngoscope into the mouth)
- Secondary outcomes included lowest SpO2 recorded, lowest HR, number of intubation attempts, duration of successful attempts, crossover to the alternative device, and correct ETT position on CXR
- Data was recorded contemporaneously by research assistants (including out-of-hours)
- After 226 were randomised, 214 neonates were underwent either VL (107, 50%) or DL and were included in the intent-to-treat analysis
- Groups were well matched at baseline with mean age 29.6 with VL vs 28.4 weeks with DL, 42% <1000g in both groups. Most intubations were performed in the NICU (64% and 77% respectively) by doctors training in paediatrics (63% and 64% respectively). A stylet was used in almost all intubation attempts.
- Results: Successful intubation on the first attempt occurred in 74% (95% CI 66-82) of the VL group compared with 45% (95% CI 35-54) of the DL group (P<0.001)
- This difference favouring VL persisted across the subgroup analyses including age < 32wks, BW < 1000g, NICU vs operative room
- The median number of attempts to achieve successful intubation was 1 (95% CI, 1-1) in the VL group and 2 (95% CI, 1-2) in the DL group
- Intubation was attempted with the non-assigned device in 3% of the VL group compared with 28% of DL group. Medial lowest SpO2 was 74% with VL and 68% with DL, median lowest HR was 153 with VL and 148 with DL. Only 1 patient in the DL group experienced oral trauma compared with none in the VL group. There was no difference in ETT positioning on chest X-ray
- Strengths:
- This trial included all neonates including those <32wks gestation and <1000g and provided new data in this population that has previously been excluded from airway trials. It provided valuable data that VL is safe and effective in this age range
- There was good protocol adherence with only 1 protocol violation recorded and data was collected contemporaneously by research assistants which adds to the internal validity of the study
- Limitations:
- Single-centre study with modest number of patients
- Clinicians and assessors were naturally aware of the group assignment
- Only one type of video laryngoscopy device was assessed (CMAC device) so results may not translate to other VL devices
- Most of the clinicians attempting the first intubation were doctors in training with presumably limited intubation experience, though this data was not collected so we can’t know for sure
- While this study was not performed in the ED, it is reasonable to conclude that similar benefit may be seen with VL use when neonatal intubation is required given the growing familiarity with VL by ED providers when intubating children and adults
- The trial was not adequately powered to report on adverse outcomes, however VL trended towards a more favourable adverse event profile anyway
References
- Prekker ME, Driver BE, Trent SA et al. DirEct versus VIdeo LaryngosCopE (DEVICE): protocol and statistical analysis plan for a randomised clinical trial in critically ill adults undergoing emergency tracheal intubation. BMJ Open. 2023 Jan 13;13(1):e068978.
- Garcia-Marcinkiewicz AG, Kovatsis PG, Hunyady AI et al. First-attempt success rate of video laryngoscopy in small infants (VISI): a multicentre, randomised controlled trial. Lancet. 2020 Dec 12;396(10266):1905-1913.
- Foglia EE, Ades A, Sawyer T, et al. Neonatal intubation practice and out- comes: an international registry study. Pediatrics 2019;143(1):e20180902.
Geraghty LE, Dunne EA, Ní Chathasaigh CM et al. Video versus Direct Laryngoscopy for Urgent Intubation of Newborn Infants. N Engl J Med. 2024 May 30;390(20):1885-1894.