Conclusion: Preoxygenation with noninvasive ventilation results in less critical hypoxia than with face mask oxygen without an apparent increase in adverse events for critically ill adults undergoing intubation
My take away: This is a practice-changing study. NIV appears safe for preoxygenation and should be considered particularly in patients who are already hypoxaemic or who have a high BMI
- Hypoxia occurs during about 10-20% of intubation episodes in the ED and ICU and is associated with adverse events including cardiac arrest and death [1]
- Preoxygenation is typically performed with face mask oxygen (so called ‘non-rebreather masks’) which can entrain ambient air reducing the inhaled FiO2 to as low as 50%, and without the provision or PEEP or ventilatory support
- Non-invasive ventilation has been proposed as the ideal preoxygenation technique however supporting data to date has been limited. While NIV mask non-compliance was previously a concern (DSI takes care of this) there have always been concerns with regards to safety, in particular haemodynamic effects from positive pressure ventilation and gastric insufflation and aspiration risk
- This was a pragmatic, multicentre, unblinded, parallel-group RCT conducted across 24 sites (7 EDs and 17 ICUs) across 15 hospitals in the US
- Eligible patients were those ≥18 yrs undergoing tracheal intubation that involved the use of sedation and a laryngoscope
- Patients were excluded if pregnant, incarcerated, were already receiving NIV, had apnoea or hyponoea, or an immediate need for tracheal intubation that precluded randomisation. Importantly, patients were also excluded if the treating clinician determined that either preoxygenation method was either necessary or contraindicated
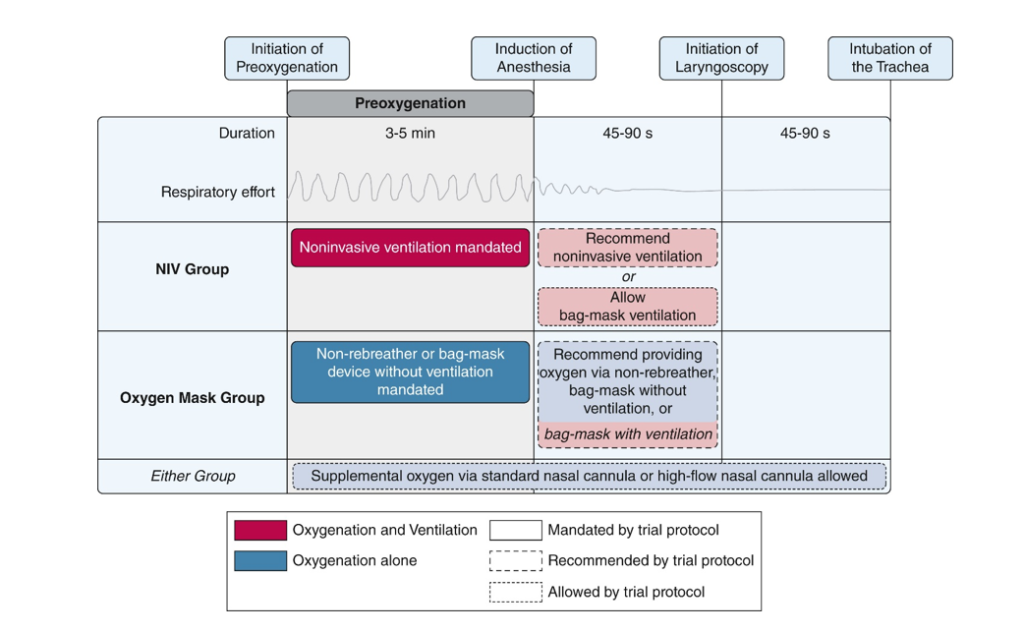
- Practice recommendations (not mandated) were given to providers for both treatment groups and included:
- For NIV: FiO2 100%, EPAP at least 5cmH20, IPAP at least 10cmH20, RR at least 10 bpm, delivered from start of preoxygenation to beginning of laryngoscopy
- For face mask oxygen: use of face mask or BVM with highest oxygen flow rate available (≥15 litres per minute), from start of preoxygenation to beginning of laryngoscopy
- Preoxygenation was performed for at least 3 minutes, if feasible
- The protocol allowed operators to provide, at their discretion, ventilation with a bag-mask device to patients in either trial group after induction of anaesthesia
- The protocol also allowed for the administration of supplemental oxygen through a standard nasal cannula or high-flow nasal cannula to the patients in either trial group during preoxygenation, during the interval between induction and initiation of laryngoscopy, and the interval between initiation of laryngoscopy and tracheal intubation
- Primary outcome was hypoxaemia during intubation, defined by an oxygen saturation of less than 85% during the interval between induction of anaesthesia and 2 minutes after tracheal intubation
- Secondary outcome was the lowest saturations recorded during this period
- Exploratory outcomes including haemodynamic events (SBP < 65 mmHg or new/increased vasopressor use) and cardiac arrest, and safety outcomes included clinical, radiographic, and physiological evidence of aspiration
- Data was collected by trained research assistants, not the clinicians involved
- Power calculations predicted 1300 patients required (650 in each group) to detect a 6% absolute difference in severe hypoxaemia
- 4567 patients were assessed for eligibility, of whom 1301 were enrolled in the trial (645 in the NIV group and 656 in the face mask group). Approximately 27% were from the ED and 73% in the ICU
- Groups had similar baseline characteristics with median age of 61, approximately 40% female in both groups and median BMIs of 27.6 and 26.6 respectively
- Altered mental status was the most common cause for need for intubation (62.3% and 59.5%) followed by sepsis (46.7% and 47.6%) and pneumonia (16.6% and 15.5%). Median APACHE II scores were 17 in both groups. Median highest FiO2 required in the hour prior to intubation was similar at 33% and 36% respectively
- There was a high level of assigned treatment provision in this pragmatic trial with 95.5% of the NIV group receiving NIV, and 98.8% of the face mask group receiving face mask oxygen. Preoxygenation was performed for at least 3 minutes in >95% of both groups
- An oxygen saturation of 95% or less at the time of induction was recorded in 8.3% in the NIV group and 17.4% in the oxygen-mask group (absolute risk difference 9.1%, 95% CI −12.7 to −5.5)
- 30.8% of the oxygen-mask group received bag-mask ventilation between induction and laryngoscopy
- Results: Hypoxaemia (SpO2 <85%) occurred in 57/624 (9.1%) in the NIV group and 118/637 (18.5%) in the oxygen-mask group (absolute risk difference 9.4%, 95% CI -13.2 to -5.6, p<0.001)
- Median lowest SpO2 was 99% in the NIV group vs 97% in the oxygen-mask group (median difference 2%; 95% CI 1 to 3)
- The treatment effect of NIV appeared to be greatest amongst patients with hyperaemic respiratory failure, a higher BMI, and a higher FiO2 requirement

- For the exploratory outcomes, SpO2 <70% was more less frequent in the NIV group (2.4% vs 5.7%, 95% CI −5.4 to −1.1) as was cardiac arrest (0.2% vs 1.1%, 95% CI -1.8 to -0.1)
- Aspiration occurred in 0.9% of the NIV group vs 1.4% of the oxygen-mask group (95% CI −1.6 to 0.7). There was no statistical difference between groups in rates of CV collapse, SBP < 65mmHg, new or increased vasopressor requirements, first-pass success, ventilator free days, ICU-free days, or in-hospital mortality
- Strengths:
- Large patient cohort that met predefined power calculation to detect a clinically meaningful benefit
- Multicentre design encompassing the breadth of critically ill patients in both the ED and ICU from a large spectrum of underlying causes adds to the external validity and generalisability of the trial
- Data was collected by research assistants and not the clinicians involved, with the primary outcome (SpO2 level) an objective, measurable data point
- While the primary outcome is not strictly patient-centred, hypoxia is highly important and a strong surrogate marker for patient safety
- Limitations:
- The primary outcome was a clinical measurement and not a patient-oriented outcome
- Patients already receiving NIV at the time of eligibility were excluded, so this dataset doesn’t inform care for those patients. However, the ongoing need and benefit of NIV in these patients prior to intubation appears readily apparent. It would be an odd decision to remove NIV from a patient already deemed to require it in favour of an oxygen-mask prior to intubation
- Probably more importantly, patients were excluded if the treating clinician determined that either NIV or oxygen-mask was either necessary or contraindicated. While legitimate contraindications to NIV exist (e.g. BOS fracture), this treating clinician determination goes some way to undermine the goal of this study (that is, to show whether NIV truly has benefit in terms of preoxygenation to support favouring its use).
- Non-compliance with NIV mask excluded many patients from this trial, but Delayed-Sequence Intubation with ketamine is a legitimate and effective method of facilitating NIV compliance for preoxygenation prior to induction which would have added valuable data to this study cohort
- Data regarding the use of apnoeic oxygenation in either (which was permitted per the treatment recommendations) was not presented, and may have had an impact on the primary outcome
- The study was not blinded (which would have been near impossible to do)
Gibbs KW, Semler MW, Driver BE, et al. Noninvasive Ventilation for Preoxygenation during Emergency Intubation. NEJM. June 2024. DOI: 10.1056/NEJMoa2313680.
https://www.nejm.org/doi/full/10.1056/NEJMoa2313680
References:
- Pfuntner A, Wier LM, Stocks C. Most frequent procedures performed in U.S. hospitals, 2011. Statistical brief no. 165. Rockville, MD: Agency for Healthcare Research and Quality, October 2013.