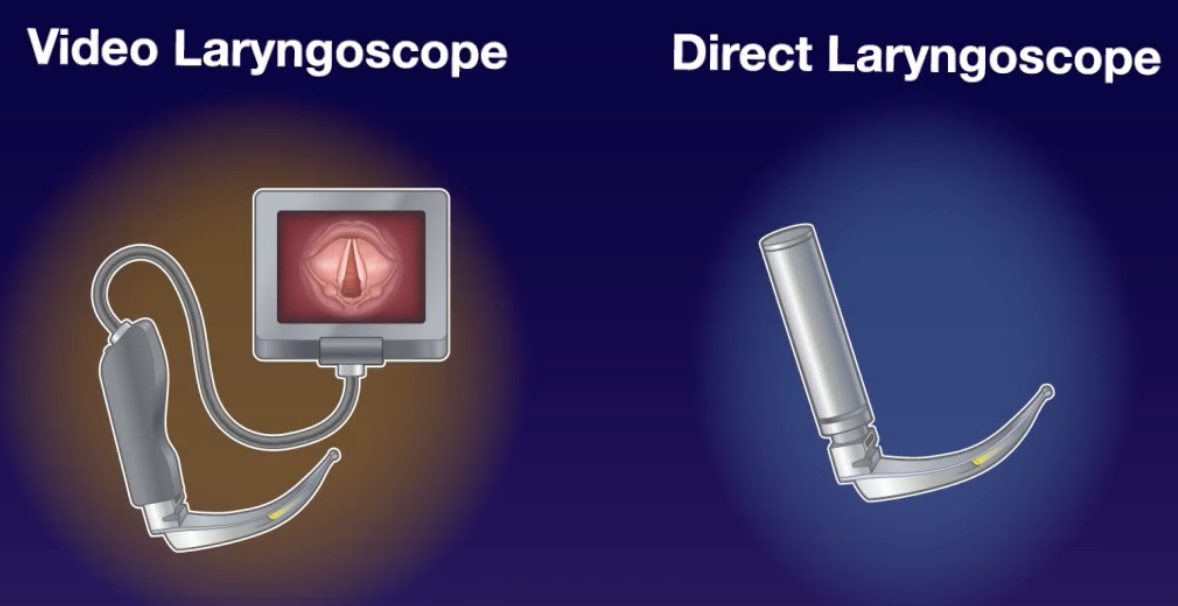
Conclusion: Video laryngoscopy results in higher rates of first-pass success when intubating critically ill adults in an Emergency Department or ICU
My take away: In this day and age, video laryngoscopy should be standard of care for all intubations. The understanding of airway anatomy and ability to facilitate teaching for learners is unparalleled. VL makes intubating easier, but always remember to make sure the basics are perfected, including appropriate patient positioning. This way if a VL device fails for any reason, it can still be used as a direct laryngoscope.
- The DEVICE trial seeks to answer the question of whether to choose VL or DL when intubating adults within the Emergency Department or ICU
- Failure to intubate the trachea on the first attempt occurs in 20 to 30% of tracheal intubations performed in the emergency department or intensive care unit (ICU) and is associated with an increased risk of life-threatening complications
- Several single-centre trials and a moderate-sized multicentre trial have been conducted to compare the outcomes when VL vs DL is used, and these trials showed differing results, including better outcomes with a VL, better outcomes with DL, and no significant differences in outcomes between the two types
- One major issue has been that most prior studies have been either retrospective observational or prospective studies randomised according to a factor other than blade type
- This was a large, multicentre, unblinded, prospective randomised trial from 7 EDs and 10 ICUs across the United States enrolling patients 18 yrs or older undergoing endotracheal intubation
- Those who were pregnant, prisoners, had an immediate need for tracheal intubation that precluded randomisation, or had a clinician-determined need for a particular device choice on first attempt were excluded
- The primary outcome was successful intubation on the first attempt, defined as the placement of an ETT in the trachea with a single insertion of a laryngoscope blade (+/- bougie) and ETT into the mouth
- The secondary outcome was a composite of severe hypoxaemia, hypotension, need for vasopressors, cardiac arrest, or death within 2 minutes after the procedure
- 1947 patients were assessed for eligibility, of whom 1420 (72.9%) were enrolled
- 3 were subsequently identified as prisoners and therefore excluded
- Patient characteristics were similar across groups, with a mean age of approximately 55 years, a mean BMI of 26.5 kg/m2
- 70% of intubations occurred in the ED
- Median number of previous intubations performed: 50 vs 50
- Resident intubators: 73% vs 71%
- Altered mental status or pneumonia being the primary indications for intubation in most cases (45% and 30%, respectively)
- Protocol adherence was high VL used in 100.0% of those randomised to the VL group, while DL was used in 98.9% of the DL group
- Results: Successful intubation on the first attempt occurred in 600 of the 705 patients (85.1%) in the VL group and in 504 of the 712 patients (70.8%) in the DL group (absolute risk difference, 14.3 percentage points; 95% CI, 9.9 to 18.7; P<0.001)
- A Grade 1 view (Cormack-Lehane) was reported in 76.3% of the VL group vs 44.7% of the DL group (absolute risk difference, 31.6 percentage points; 95% confidence interval [CI], 26.7 to 36.6)
- There was no significant difference in the composite secondary outcome between groups
- The study was stopped early with these results following a planned interim analysis
- Strengths:
- Very well done RCT with robust study design
- Multicentre study that increases external validity
- Reflective of real work practise with decision of blade type (standard geometry vs hyperangulated) left up to treating clinician
- Limitations:
- Relative inexperience group of intubators limits generalisability to more experienced clinicians, supported by the fact that the between group difference decreased to 5.9% among operators with >100 prior intubations (still favouring VL)
- There was a high baseline usage of VL compared to DL which may have affected performance in the DL group due to unfamiliarity with the device
Reference: Prekker ME, Driver BE, Trent SA, et al. Video versus Direct Laryngoscopy for Tracheal Intubation of Critically Ill Adults. N Engl J Med. 2023 Aug 3;389(5):418-429.
Full article: https://www.nejm.org/doi/pdf/10.1056/NEJMoa2301601