Conclusion: Both DSED and VC defibrillation were associated with increased rates of survival to hospital discharge and VF termination when compared to standard anterolateral pad shocks for patients with refractory out-of-hospital cardiac arrest.
- This was a cluster-randomized trial with crossover every 6 months among six Canadian paramedic services to evaluate defibrillation strategies for refractory VF
- Refractory VF was defined as ongoing VF or pulseless VT despite 3 standard anterolateral pad shocks
- The interventions compared were:
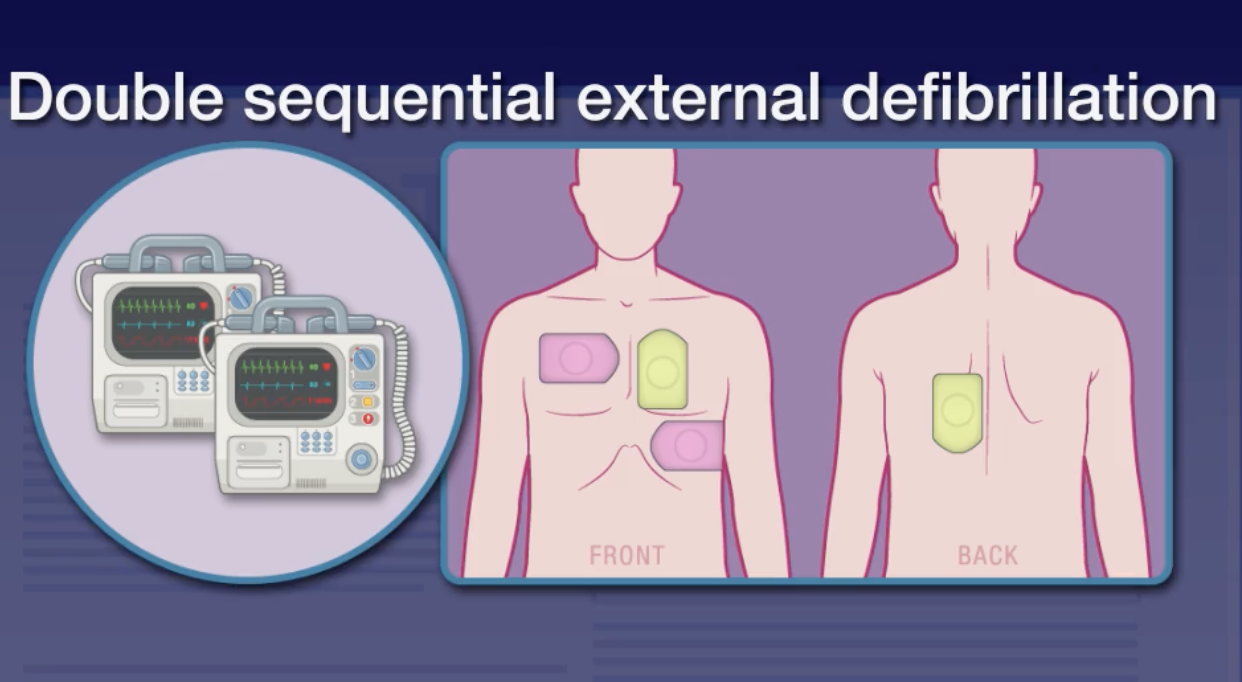
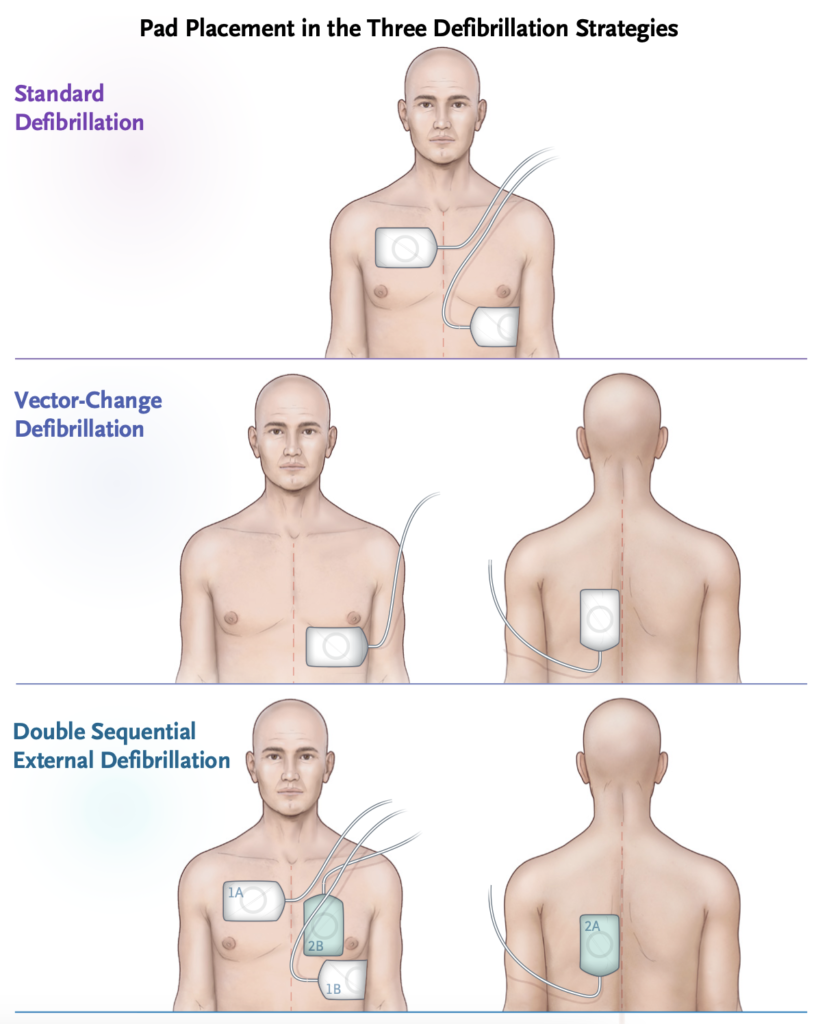
- Double sequential external defibrillation (DSED) – sequential shocks from two defibrillators 1 second apart
- Vector-change defibrillation (VC) – switching defibrillation pads to an anterior–posterior position
- Standard anterolateral pad placement
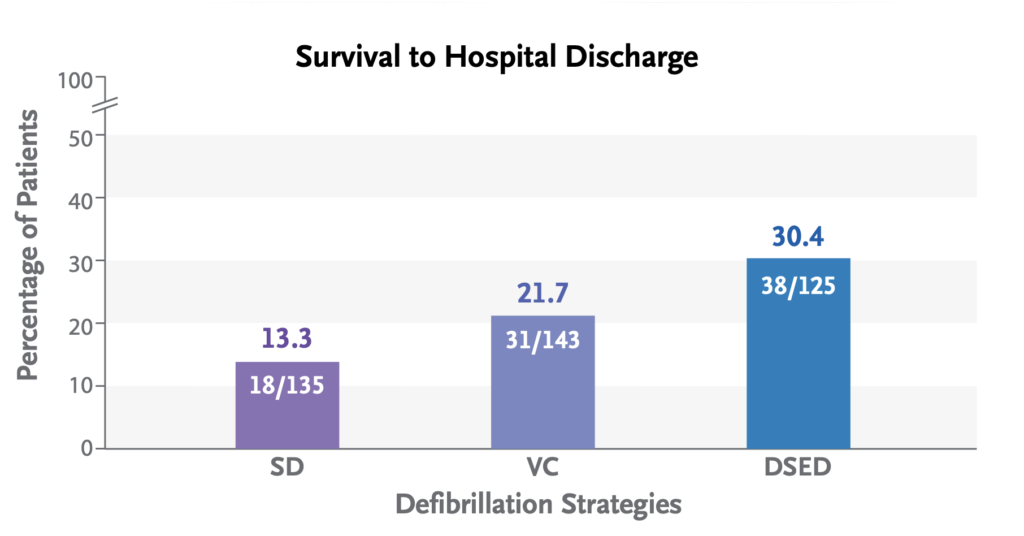
- Primary outcome was survival to hospital discharge. Secondary outcomes included termination of VF, return of spontaneous circulation, and a good neurologic outcome at hospital discharge (mRankin =< 2)
- 405 patients were enrolled before the trial was stopped because of the COVID pandemic (the target sample size was 930 patients) and allocated:
- DSED – 125 patients (30.9%)
- VC – 144 patients (35.6%)
- Standard defibrillation – 136 patients (33.6%)
- Protocol violations occurred at a high rate: 107 of 125 patients in the DSD arm received DSD, and 113 of 144 patients in the VC arm received a VC shock. The data are presented as intent to treat.
- Survival to hospital discharge was more common in the DSED group than in the standard group (30.4% vs. 13.3%; relative risk, 2.21; 95% confidence interval [CI], 1.33 to 3.67) and more common in the VC group than in the standard group (21.7% vs. 13.3%; relative risk, 1.71; 95% CI, 1.01 to 2.88).
- DSED but not VC defibrillation was associated with a higher percentage of patients having a good neurologic outcome than standard defibrillation (relative risk, 2.21 [95% CI, 1.26 to 3.88] and 1.48 [95% CI, 0.81 to 2.71], respectively).
- Strengths:
- Crossover study design decreases risk of bias from paramedic teams performing at different levels
- There was a standardised protocol for implementation of standard resuscitation, VC and DSED
- Limitations:
- As the trial was stopped early, it’s possible the treatment effect is overestimated
- Paramedics were not blinded and therefore might have worked harder on patients receiving a new treatment than patients receiving more of the same treatment
- There was a high rate of protocol violations, and the statistical significance disappeared in an analysis according to the treatment actually received (per protocol), although the trend favouring DSD and VC remained.
Full article: https://www.nejm.org/doi/pdf/10.1056/NEJMoa2207304
Reference: Cheskes S, Verbeek PR, Drennan IR, McLeod SL, Turner L, Pinto R, Feldman M, Davis M, Vaillancourt C, Morrison LJ, Dorian P, Scales DC. Defibrillation Strategies for Refractory Ventricular Fibrillation. N Engl J Med. 2022 Nov 24;387(21):1947-1956.