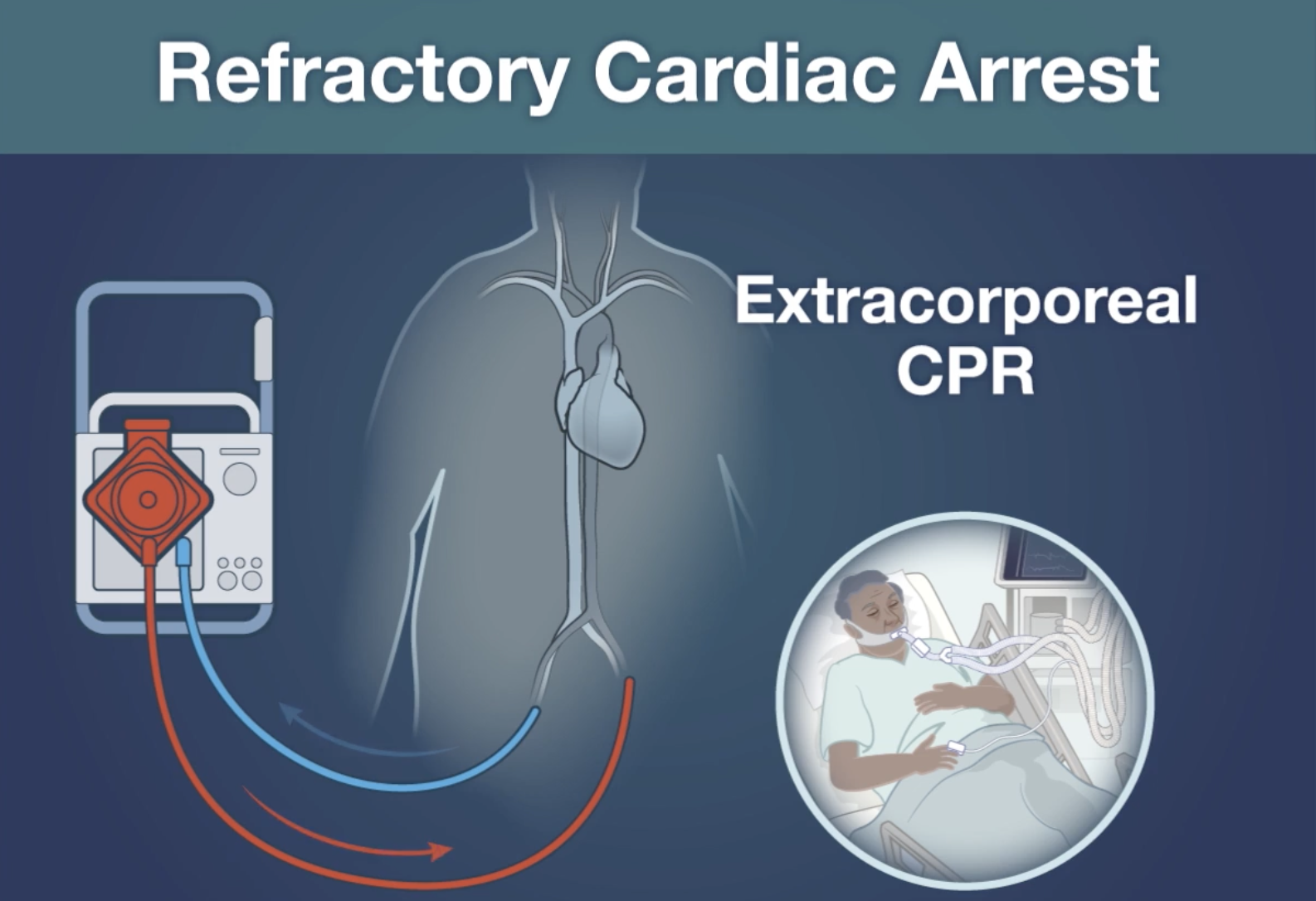
Conclusion: Early use of Extracorporeal-CPR for refractory out of hospital cardiac arrest did not result in increased survival with favourable neurologic outcome
- This study (the largest randomised trial on E-CPR to date) was a multicenter, randomised controlled trial conducted in the Netherlands where patients with an out-of-hospital cardiac arrest were assigned to receive extracorporeal CPR or conventional CPR (standard advanced cardiac life support)
- Eligible patients were:
- Aged between 18 and 70 years of age
- Had received bystander CPR
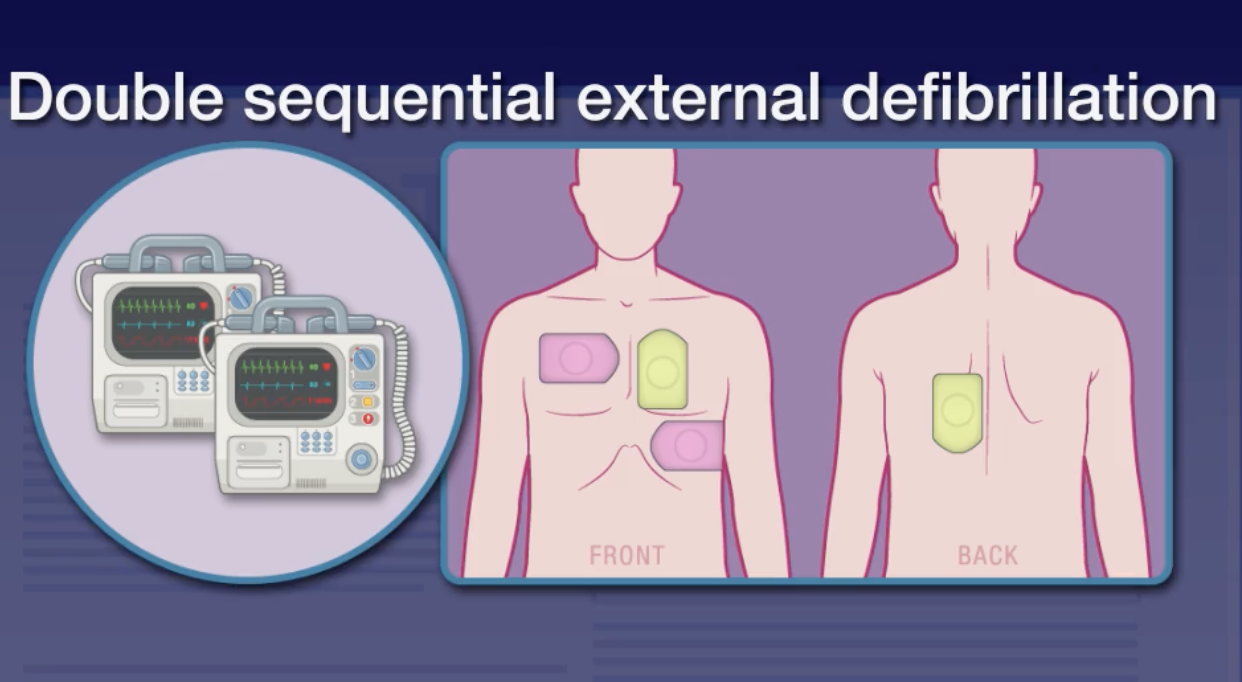
- Had an initial ventricular arrhythmia
- Failed to have ROSC after 15 minutes CPR
- Exclusion criteria included patients with a known severe or terminal disease (e.g. advanced cancer), pregnancy, poor baseline neurologic function, and those who had ROSC within 15 minutes
- Enrolment occurred either during transport (EMS teams were blinded en route) or on hospital arrival
- Patients >60 minutes on arrival could still be included (despite it being an exclusion criteria at the time of randomisation)
- Primary outcome was survival with a favourable neurologic outcome at 30 days, defined as a Cerebral Performance Category score of 1 or 2 (normal or disabled but independent)
- The study was powered to detect a 22% absolute difference in the primary outcome
- Secondary outcomes included:
- Duration of CPR before return of circulation
- Total duration of CPR
- ICU and hospital length of stay
- 30-day and 6-month survival
- 6-month Cerebral Performance Category score
- Reason for discontinuation of treatment
- Duration of mechanical ventilation
- A total of 160 patients were randomly assigned to receive extracorporeal CPR or conventional CPR; 26 of the patients who underwent randomization did not meet the inclusion criteria at hospital admission and were excluded. The final population was 70 patients in the extracorporeal-CPR group and 64 patients in the conventional-CPR group
- Only 46/70 (66%) of the E-CPR group actually successfully received therapy due to various reasons (18 had ROSC, “logistic failure” or cessation of treatment, while 6 had unsuccessful cannulations)
- 52/64 (81%) of the conventional CPR-group received standard therapy (9 had ROSC, 3 crossed over to receive E-CPR – all died) 64 assigned to conventional CPR
- The groups were well balanced at baseline in terms of age, gender, comorbidities, cardiac arrest details and cause of arrest
- Results: Survival at 30 days with a Cerebral Performance Category score of 1 or 2 had occurred in 14 of the 70 patients (20%) in the extracorporeal-CPR group and in 10 of the 62 patients with data (16%) in the conventional-CPR group (odds ratio 1.4; 95% confidence interval, 0.5 to 3.5; P=0.52)
- E-CPR was associated with a higher proportion of patients who survived until admission to the ICU than conventional CPR (57 (81%) vs 23 (36%)), and with this substantially higher resource utilisation
- No difference in survival to hospital discharge or 6-month survival with favourable neurologic outcome
- No E-CPR survivors had poor neurologic outcomes
- Strengths:
- This is the largest randomised trial examining E-CPR to date
- Study groups appeared well matched
- Minimal loss to follow up
- Limitations:
- ROSC post randomisation and cannulation failure meant that only 46/70 (66%) of the E-CPR group actually received E-CPR
- While EMS were blinded to randomisation, the treating medical teams were not and they could withdraw patients
- Note though that this generally favours the intervention group anyway
- As the authors note, the lack of standardisation of protocols for E-CPR may be a limitation, but this may also increase the generalisability of the resuscitation procedures and E-CPR
- These median intervals for commencement of E-CPR are longer than those in both the ARREST trial and the PRAGUE OHCA study and may reflect differences in such factors as team experience, logistics, and caseload
There are 2 previous randomised controlled trials examining E-CPR for refractory OHCA:
- The ARREST trial (Yannopolous et al., Lancet 2020) included 30 patients with OHCA with VT/VF as the initial rhythm. Survival to hospital discharge was higher with E-CPR: 6/14 (43%) vs 1/15 (7%) (posterior probably of benefit 0.98%). This trial was stopped early due to benefit.
- The PRAGUE OHCA trial (Behlolavek et al., JAMA 2022) included 260 patients with OHCA with VT/VF and PEA and reported a trend of benefit but no statistical significance in increased good neurological outcome at day 180 (32% vs 22% P=0.09). This trial was stopped early due to futility.
References:
INCEPTION: Suverein MM, Delnoij TSR, Lorusso R, et al. Early Extracorporeal CPR for Refractory Out-of-Hospital Cardiac Arrest. N Engl J Med. 2023 Jan 26;388(4):299-309.
ARREST: Yannopoulos D, Bartos J, Raveendran G, et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): a phase 2, single centre, open-label, randomised controlled trial. Lancet. 2020 Dec 5;396(10265):1807-1816.
PRAGUE OHCA: Prague OHCA Study Group. Effect of Intra-arrest Transport, Extracorporeal Cardiopulmonary Resuscitation, and Immediate Invasive Assessment and Treatment on Functional Neurologic Outcome in Refractory Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial. JAMA. 2022 Feb 22;327(8):737-747.